Projected Smoking-Related Deaths Among Youth -- United States
Download PDF Version What is PDF?
Reported by the following BRFSS coordinators: J Durham, MPA, Alabama; P Owen, Alaska; B Bender, Arizona; J Senner, PhD, Arkansas; B Davis, PhD, California; M Leff, MSPH, Colorado; M Adams, MPH, Connecticut; F Breukelman, Delaware; C Mitchell, District of Columbia; D McTague, MS, Florida; E Pledger, MPA, Georgia; J Cooper, MA, Hawaii; C Johnson, MPH, Idaho; B Steiner, MS, Illinois; N Costello, MPA, Indiana; P Busick, Iowa; M Perry, Kansas; K Asher, Kentucky; R Meriwether, MD, Louisiana; D Maines, Maine; A Weinstein, MA, Maryland; D Brooks, MPH, Massachusetts; H McGee, MPH, Michigan; N Salem, PhD, Minnesota; S Loyd, Mississippi; J Jackson-Thompson, PhD, Missouri; P Smith, Montana; S Huffman, Nebraska; E DeJan, MPH, Nevada; K Zaso, MPH, New Hampshire; G Boeselager, MS, New Jersey; W Honey, New Mexico; T Melnik, DrPH, New York; G Lengerich, VMD, North Carolina; J Kaske, MPH, North Dakota; R Indian, MS, Ohio; N Hann, MPH, Oklahoma; J Grant-Worley, MS, Oregon; L Mann, Pennsylvania; J Hesser, PhD, Rhode Island; J Ferguson, DrPh, South Carolina; M Gildemaster, South Dakota; D Ridings, Tennessee; R Diamond, MPH, Texas; R Giles, Utah; R McIntyre, PhD, Vermont; J Stones, Virginia; K Wynkoop-Simmons, PhD, Washington; F King, West Virginia; E Cautley, MS, Wisconsin; M Futa, MA, Wyoming. P Mowery, MA, J Shulman, PhD, Battelle Memorial Institute, Baltimore, Maryland. Epidemiology Br, Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion, CDC.
Source: Centers for Disease Control and Prevention, Projected Smoking-Related Deaths Among Youth -- United States, MMWR, 45(44);971-974, November 8, 1996
Public Domain
Table of Contents (TOC)
Article: Projected Smoking-Related Deaths Among Youth -- United StatesEditorial Note
Tables
References


 On August 23, 1996, the Food and Drug Administration (FDA)
issued a regulation restricting the sale and distribution
of cigarettes and smokeless tobacco to children and teenagers
to reduce the number of youth who use these products and
to reduce the life-threatening consequences associated with
tobacco use.1 Despite widespread efforts to educate U.S.
youths about the health consequences associated with smoking,2 the prevalence of smoking among this group has been
increasing since 1992.3 To assess the need for continued
public health efforts to prevent nicotine addiction, CDC
used a model including data from the Behavioral Risk Factor
Surveillance System (BRFSS) to project the future impact
of smoking on the health of children and teenagers. This
report presents the findings of the analysis, which indicate
that, if current tobacco-use patterns persist, an estimated
5 million persons who were aged 0-17 years in 1995 will
die prematurely from a smoking-related illness.
On August 23, 1996, the Food and Drug Administration (FDA)
issued a regulation restricting the sale and distribution
of cigarettes and smokeless tobacco to children and teenagers
to reduce the number of youth who use these products and
to reduce the life-threatening consequences associated with
tobacco use.1 Despite widespread efforts to educate U.S.
youths about the health consequences associated with smoking,2 the prevalence of smoking among this group has been
increasing since 1992.3 To assess the need for continued
public health efforts to prevent nicotine addiction, CDC
used a model including data from the Behavioral Risk Factor
Surveillance System (BRFSS) to project the future impact
of smoking on the health of children and teenagers. This
report presents the findings of the analysis, which indicate
that, if current tobacco-use patterns persist, an estimated
5 million persons who were aged 0-17 years in 1995 will
die prematurely from a smoking-related illness.
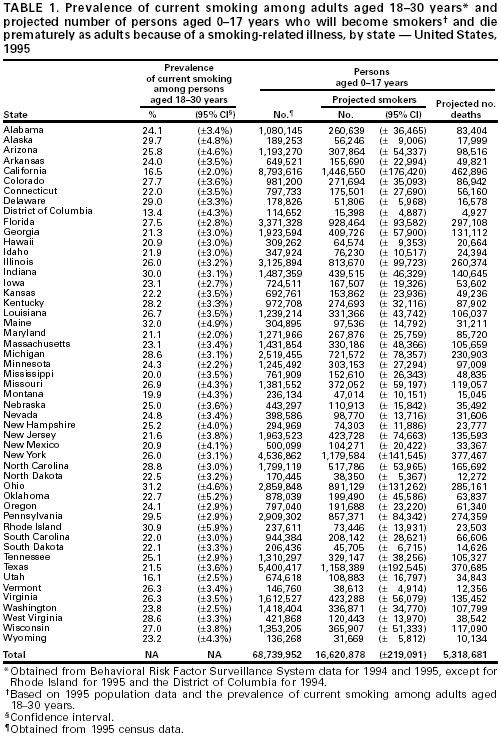
State-specific data on the prevalence of current smoking among adults aged 18-30 years in all 50 states and the District of Columbia were obtained from the BRFSS for 1994 and 1995.4 Current smokers were respondents who reported having smoked 100 cigarettes during their lifetimes and who reported currently smoking. Because the prevalence of smoking in a birth cohort peaks during early adulthood,2 the average prevalence of smoking among adults aged 18-30 years for each state during 1994-1995 was used to estimate the future prevalence of smoking during early adulthood for the birth cohorts currently aged 0-17 years. The number of persons aged 0-17 years in 1995 in each state was obtained from U.S. census reports5 and was multiplied by the estimated prevalence of future smoking to calculate the estimated number of youths who may become regular smokers in each state. Overall, the estimated number of future smokers among the cohort of persons who were aged 0-17 years in 1995 was 16,620,878 for the United States (range: 15,398 {District of Columbia} to 1,446,550 {California}) (Table_1).
 The projected number of smoking-related deaths among youth
smokers was based on the combined estimates of young adult
smokers who continue to smoke throughout their lifetimes
and estimates of premature death attributable to smoking
among continuing smokers6 and among those who quit after
age 35 years.7 Based on data from the 1986 National Mortality
Followback Survey (NMFS), 55% (95% confidence interval {CI}=
plus or minus 1%) of persons who had ever smoked greater
than or equal to 100 cigarettes during their lifetimes continued
to smoke until 1 year before their deaths, and 45% (95%
CI= plus or minus 1%) quit smoking earlier in their adult
lives (CDC, unpublished data, 1995). Based on data from
long-term cohort studies, an estimated 50% of deaths among
continuing smokers will be attributable to smoking.6
Although estimates of the number of smoking-attributable
deaths among former smokers range from 10% to 37%, a conservative
estimate of 10% was used in this analysis (CDC, unpublished
data, 1996).7 The future probability of smoking-attributable
mortality (PSAM) among youth was computed to be PSAM={(0.55
X 0.5)+(0.45 X 0.1)}=0.32. Estimates for the variance of
the two smoking-attributable fractions (50% and 10%) within
the PSAM were computed from the Cancer Prevention Study
II.8 These two variances were combined with the variances
for the probabilities of continued smoking or quitting using
a Taylor Series approximation method, which yielded an estimate
of 0.00422 of the relative error of the PSAM. To reflect
the uncertainty of the multiple assumptions about future
smoking and mortality patterns, this error estimate for
the PSAM was increased by a factor of 2.5, yielding an estimated
standard error of 0.0106.
The projected number of smoking-related deaths among youth
smokers was based on the combined estimates of young adult
smokers who continue to smoke throughout their lifetimes
and estimates of premature death attributable to smoking
among continuing smokers6 and among those who quit after
age 35 years.7 Based on data from the 1986 National Mortality
Followback Survey (NMFS), 55% (95% confidence interval {CI}=
plus or minus 1%) of persons who had ever smoked greater
than or equal to 100 cigarettes during their lifetimes continued
to smoke until 1 year before their deaths, and 45% (95%
CI= plus or minus 1%) quit smoking earlier in their adult
lives (CDC, unpublished data, 1995). Based on data from
long-term cohort studies, an estimated 50% of deaths among
continuing smokers will be attributable to smoking.6
Although estimates of the number of smoking-attributable
deaths among former smokers range from 10% to 37%, a conservative
estimate of 10% was used in this analysis (CDC, unpublished
data, 1996).7 The future probability of smoking-attributable
mortality (PSAM) among youth was computed to be PSAM={(0.55
X 0.5)+(0.45 X 0.1)}=0.32. Estimates for the variance of
the two smoking-attributable fractions (50% and 10%) within
the PSAM were computed from the Cancer Prevention Study
II.8 These two variances were combined with the variances
for the probabilities of continued smoking or quitting using
a Taylor Series approximation method, which yielded an estimate
of 0.00422 of the relative error of the PSAM. To reflect
the uncertainty of the multiple assumptions about future
smoking and mortality patterns, this error estimate for
the PSAM was increased by a factor of 2.5, yielding an estimated
standard error of 0.0106.
Based on application of this PSAM to the state-specific estimates of potential smokers, the overall number of potential future smoking-attributable deaths among persons aged 0-17 years during 1995 was 5,318,681 for the United States (range: 4927 {District of Columbia} to 462,896 {California}) (Table_1). Based on the estimated PSAM variance and the state-specific sampling errors from the BRFSS estimates of smoking prevalence, the estimated number of smoking-related deaths for the United States overall was predicted to vary by less than or equal to 160,000 deaths.
The findings in this report indicate that, if current patterns of smoking behavior persist, an estimated 5 million U.S. persons who were aged 0-17 years in 1995 could die prematurely from smoking-related illnesses. These projected patterns of smoking and smoking-related deaths could result in an estimated $200 billion (in 1993 dollars) in future health-care costs (i.e., $12,000 per smoker)9 and approximately 64 million years of potential life lost (i.e., 12-21 years per smoking-related death),6, 9, 10 underscoring the need for intensifying efforts to prevent smoking initiation among youth.
 The projection method used in this analysis is subject to at least
three limitations. First, although this method has been recommended
for estimating future tobacco-related deaths in developed countries,6 alternative methods may be more precise (e.g., life-table procedures
used to project future disease-specific outcomes, particularly lung
cancer). Second, this method assumes that future smoking patterns and
smoking-related disease rates will be similar to those observed in recent
generations. However, future patterns may differ: for example, the estimates
of future smoking prevalence in this analysis may be underestimated
because smoking prevalences among teenagers have been increasing in
recent years.3 Third, the estimated risks for smoking-attributable
death and the smoking-attributable fractions among quitters (i.e., 10%)
and continuing smokers (i.e., 50%) are based on studies of adults who
began smoking during the mid 1900s.6, 7 More recent data indicate
that relative risks of smoking for more recent birth cohorts of both
men and women have been increasing rather than decreasing.8 Factors
related to changes in the intensity and duration of smoking may account
in part for the substantial increase in the relative risks of smoking
from the 1960s to the 1980s (e.g., relative risks of lung cancer increased
from 11.4 to 22.4 for men and from 2.7 to 11.9 for women).8 These
increases in risk occurred despite changes in the composition of tobacco
products commonly smoked, including the widespread adoption of filter-tipped,
potentially lower "tar" cigarettes.8 While future changes in tobacco
products could reduce health risks associated with smoking, smoking
intensity and duration are likely to remain the major predictors of
future risk.8 Therefore, unless U.S. persons who were aged 0-17 years
during 1995 and who are current or potential smokers alter their future
smoking behavior relative to patterns of previous generations (e.g.,
smoke fewer cigarettes per day or quit earlier in life), the relative
risks of smoking probably will remain high.
The projection method used in this analysis is subject to at least
three limitations. First, although this method has been recommended
for estimating future tobacco-related deaths in developed countries,6 alternative methods may be more precise (e.g., life-table procedures
used to project future disease-specific outcomes, particularly lung
cancer). Second, this method assumes that future smoking patterns and
smoking-related disease rates will be similar to those observed in recent
generations. However, future patterns may differ: for example, the estimates
of future smoking prevalence in this analysis may be underestimated
because smoking prevalences among teenagers have been increasing in
recent years.3 Third, the estimated risks for smoking-attributable
death and the smoking-attributable fractions among quitters (i.e., 10%)
and continuing smokers (i.e., 50%) are based on studies of adults who
began smoking during the mid 1900s.6, 7 More recent data indicate
that relative risks of smoking for more recent birth cohorts of both
men and women have been increasing rather than decreasing.8 Factors
related to changes in the intensity and duration of smoking may account
in part for the substantial increase in the relative risks of smoking
from the 1960s to the 1980s (e.g., relative risks of lung cancer increased
from 11.4 to 22.4 for men and from 2.7 to 11.9 for women).8 These
increases in risk occurred despite changes in the composition of tobacco
products commonly smoked, including the widespread adoption of filter-tipped,
potentially lower "tar" cigarettes.8 While future changes in tobacco
products could reduce health risks associated with smoking, smoking
intensity and duration are likely to remain the major predictors of
future risk.8 Therefore, unless U.S. persons who were aged 0-17 years
during 1995 and who are current or potential smokers alter their future
smoking behavior relative to patterns of previous generations (e.g.,
smoke fewer cigarettes per day or quit earlier in life), the relative
risks of smoking probably will remain high.
FDA has issued regulations to restrict youth access to tobacco and to reduce the appeal of cigarette advertising among youths and has issued a proposal to require a program to educate youths about the health consequences associated with tobacco use.1 Because smoking-related deaths are preventable,1, 9 public health efforts should emphasize both prevention of smoking initiation in the youngest birth cohorts2 and cessation as early as possible among youth who already have started smoking.6, 7
1. Kessler DA, Witt AM, Barnett PS, et al. The Food and Drug Administration’s regulation of tobacco products. N Engl J Med 1996;335:988-94.
2. US Department of Health and Human Services. Preventing tobacco use among young people: a report of the Surgeon General. Atlanta, Georgia: US Department of Health and Human Services, Public Health Service, CDC, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 1994.
3. Johnston L, Bachman J, O’Malley P. Cigarette smoking among American teens rises again in 1995. Ann Arbor, Michigan: University of Michigan News and Information Service, December 11, 1995.
4. Frazier EL, Franks AL, Sanderson LM. Behavioral risk factor data. In: CDC. Using chronic disease data: a handbook for public health practitioners. Atlanta, Georgia: US Department of Health and Human Services, Public Health Service, CDC, 1992.
5. Bureau of the Census. Population estimates and population distribution branches. Washington, DC: US Department of Commerce, Economics and Statistics Administration, Bureau of the Census, 1995.
6. Peto R, Lopez AD, Boreham J, et al. Mortality from smoking in developed countries, 1950-2000: indirect estimates from national vital statistics. New York: Oxford University Press, 1994.
7. Mattson ME, Pollack ES, Cullen JW. What are the odds that smoking will kill you? Am J Public Health 1987;77:425-31.
8. Thun MJ, Day-Lally CA, Calle EE, Flanders WD, Heath CW. Excess mortality among cigarette smokers: changes in a 20-year interval. Am J Public Health 1995;85:1223-30.
9. US Department of Health and Human Services. For a healthy nation: returns on investment in public health. Washington, DC: US Department of Health and Human Services, Public Health Service, 1995.
10. CDC. Cigarette smoking-attributable mortality in years of potential life lost -- United States, 1990. MMWR 1993;42:645-9.